Closure of Big Nasal Septal Hole

Many surgical techniques have been defined for repair of nasal septal perforations, but the results are often insufficient for large perforations (for complete closure). Permanent millimetric repair of the defect in large perforations is not always possible. It may be necessary to remove cartilage tissue from other areas such as the ear or the ribs and use it as a graft. Septal perforation is also affected by the method used during repair and intervention, as well as by the patient's pre- and post-operative care. The open approach is thought to be more likely to provide perforation repair in cases of large septal perforations, dominating the perforation margin and providing routine surgical dissection.
Closure Nasal Septal Perforation Using Rib Cartilage Technical Detailed Explanation With Video
Video description: As a result of the examination of the patient who was found to have nasal septum perforation after the correction of the previous septum deviation in a different clinic, a large nasal septum hole with a diameter of 4x5 cm was detected and the patient was planned to repair the nasal septum perforation using rib cartilages under general anesthesia.
Operation description: After the local anesthetic injection, a midcolumellar incision was made. The alar cartilages were dissected and the nasal septum was dissected vertically in the midline. The dead epithelial layer at the edges of the perforation was removed with a scalpel. As seen in the video and the photos below, cartilage grafts of several mm thickness obtained from the rib cartilage were reversed and sutured end-to-end. In this way, cartilage larger than the size of the perforation was grafted. It was seated on the perforation in the vertical plane and its edges were sutured to the septal mucosa with 4/0 vicryl. Alar cartilages were sutured with 4/0 vicryl. The skin incision in the columella was sutured with 5/0 rapid vicryl. Internal silicone splints were placed in both nasal cavities and fixed to the anterior part of the nasal septum with 3/0 prolene. The nose was bandaged only with tapes.
 |
| In the photo above, it is seen that the perforation is completely closed with the cartilage graft, and there is no hole left. The fact that the cartilage graft is larger than the perforation and has a large contact surface to the mucosa may affect the success of the surgery. |
{kind=link}
 |
| The photo above shows how the cartilage grafts from the ribs are stitched on top of each other and end to end. Usually inverted suturing can reduce the risk of later rib cartilage bending. |
{kind=link}
 |
| The photograph above shows the image after the cartilage graft has been placed in the nasal septum perforation and sutured to the marginal mucosa. |
{kind=link}
 |
| The photograph above shows the image after the cartilage graft has been placed in the nasal septum perforation and sutured to the marginal mucosa. |
{kind=link}
 |
| In the photograph above, the image after the cartilage graft was placed in the nasal septum perforation of the cartilage graft and the tapes placed on the nose after the operation was terminated are seen. |
{kind=link}
 |
| The tomography section above shows the hole - perforation (red arrows) in the nasal septum. |
There are many different techniques that can be used in the repair of nasal septum perforation. In addition to techniques such as local mucosal flap techniques, the use of membrane and membrane products with different medical purposes, the use of temporal fascia, vomer and ethmoid perpendicular plate, there are also graft applications using inferior and middle turbinate, which I do not prefer (the technique I wrote at this end is one of the techniques I dislike because of permanently changing the anatomy of the nose, disabling the turbinates). I also do not prefer to use a nasal septal button, which is a temporary solution and can cause an increase in the diameter of the perforation.
Link group where you can read the articles published on this website about nasal septum perforation >> https://www.ent-istanbul.com/search?q=nasal+septum+perforation
After Large Nasal Septum Perforation Closure Operation, Rifampicin + Saline Irrigation
After the closure of the wide nasal septum perforation, I usually remove the internal silicone splints after 2-3 months so that the cartilage grafts placed in the nose do not come into direct contact with the air. Here, in order to keep the silicones clean and prevent infection in the surgical area, our patients are advised to mix rifampisi ampoule (250 mg) and 500 ml of istonic sterile serum, to irrigate the inside of the nose with this mixture at least 3 times a day (can be sprayed into the nose with a 20 ml injector), and then to reconstitute the inside of the nose. We recommend irrigation with normal saline or ocean water sprays. The rifampicin + isotonic serum mixture used inside the nose can be stored in the refrigerator for 3 days, after which it is appropriate not to use and discard the remaining amount. After the septum perforation repair operation, classical nasal moisturizing drops and sprays may increase the risk of infection in the nose, so I recommend using eye ointments containing antibiotics inside the nose and outside the silicones. After approximately 3 months of irrigation with antibiotic serum, we remove the internal silicone plinths and we can evaluate the surgical success with endoscopic examination.
Repair of Large Septum Perforation With Rib Cartilage Cost in Istanbul
In large septal perforation repairs, the total cost of the procedure may vary between 4500 - 6000 US Dollars (including 1 day hospitalization, blood tests and materials) depending on the hospitals, materials used and grafts. Small perforation repair can be more affordable because of less operation time and materials used.
Nasal Septal Perforation, Reciprocal Airflow Through the Hole in the Septum, and Altered Airflow
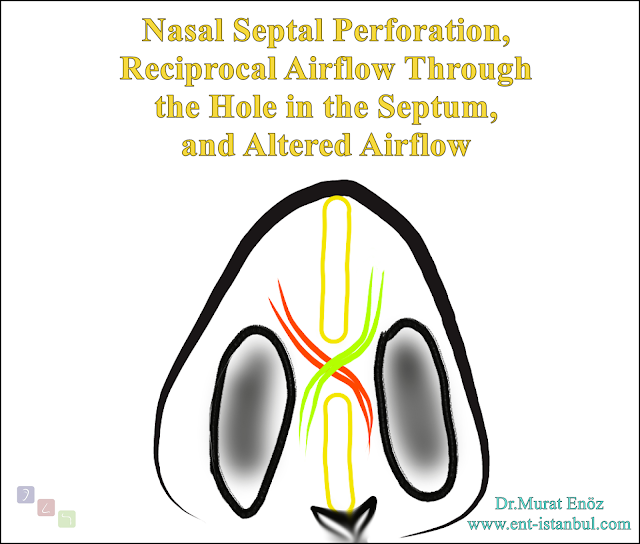
As in the animation photo above, when a hole occurs in the nasal septum, the right and left nasal cavities, which are normally two separate cavities, become directly connected to each other. In the areas around the edges, olark drying, crusting, and hole-wide growth may occur due to accelerated air passage. When this hole is small and located close to the front, the airflow through it accelerates and a "whistling sound" may occur. A whistling sound is also less likely when a nasal septal perforation is posterior and large (as well as posterior nasal septal perforations are less pronounced than anterior perforations). You can check the link about it >> The Whistle of Nose Video - Nasal Septum Perforation - Before and After Treatment
Murat Enoz, MD, Otorhinolaryngology, Head and Neck Surgeon - ENT Doctor in Istanbul
Private Office:
Address: İncirli Cad. No:41, Kat:4 (Dilek Patisserie Building), Postal code: 34147, Bakırköy - İstanbul
Appointment Phone: +90 212 561 00 52
Appointment Phone: +90 212 561 00 52
Fax: +90 212 542 74 47

Comments
Post a Comment